

Since the detection of the first positive case of coronavirus in January 2020, Nepal suffered greatly by the loss of human lives as the number of cases rose to 795,061 with 11,135 deaths by the end of September 2021. The country has projected US$1.26 billion for its national relief programme, Nepal heavily relies on its neighbours- India and China- to fill the gap in addition to other international development partners. US$452.8 million is allocated to vaccinate 71 per cent of the population, the target is still under 30 percent. No doubt, COVID-19 has weakened Nepal’s ambition of prosperity as the pandemic continues posing a serious threat to safety and security of the people and society.
.
SARS-CoV-2, commonly known as COVID-19 was first reported in Wuhan in China and posed a global threat to the humankind. The pandemic has severely affected Nepal. As of 30 September 2021, there were over 795,061 confirmed cases of COVID in Nepal with 765,758 recovered cases and 11,135 deaths (MoHP, 2021)[1]. Of the seven provinces, Bagmati Province suffers from the highest number of COVID-19 cases (Figure 1), and the highest number of deaths from the pandemic, 42 per cent of the total death in the country. Of the 77 districts, Kathmandu district also reported the highest number of human casualties (2,144 of 11,135 across the country), followed by Lalitpur (667), and Bhaktapur (425).
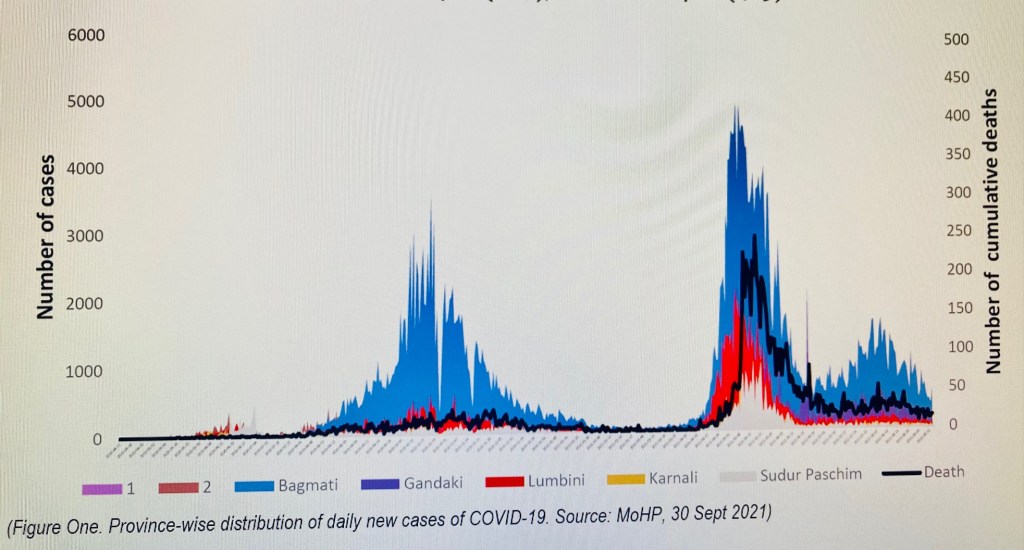
(Figure One. Province-wise distribution of daily new cases of COVID-19. Source: MoHP, 30 Sept 2021)
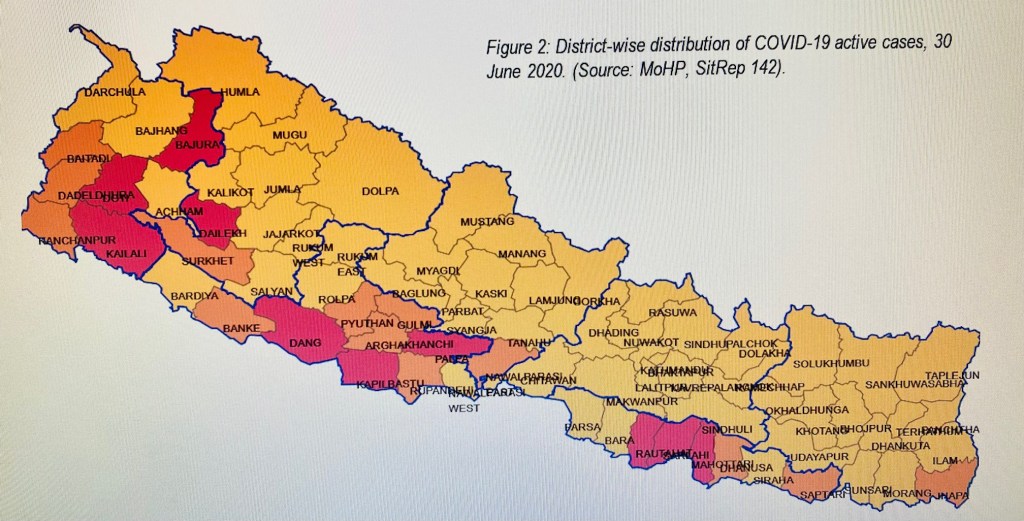
The first positive case of SARS-CoV-2 in Nepal was reported in a Nepalese student returning from Wuhan, China on 23 January 2020[2]. The case did not have a significant increase until the end of June. A dramatic surge in COVID-19 cases was reported after July (2020) to September (2020). While 228,341 RT-PCR tests resulting to 13,564 positive cases of COVID-19 with a 5.9 per cent cumulative positivity rate and 29 deaths by the end of June 2020 (Figure 2).
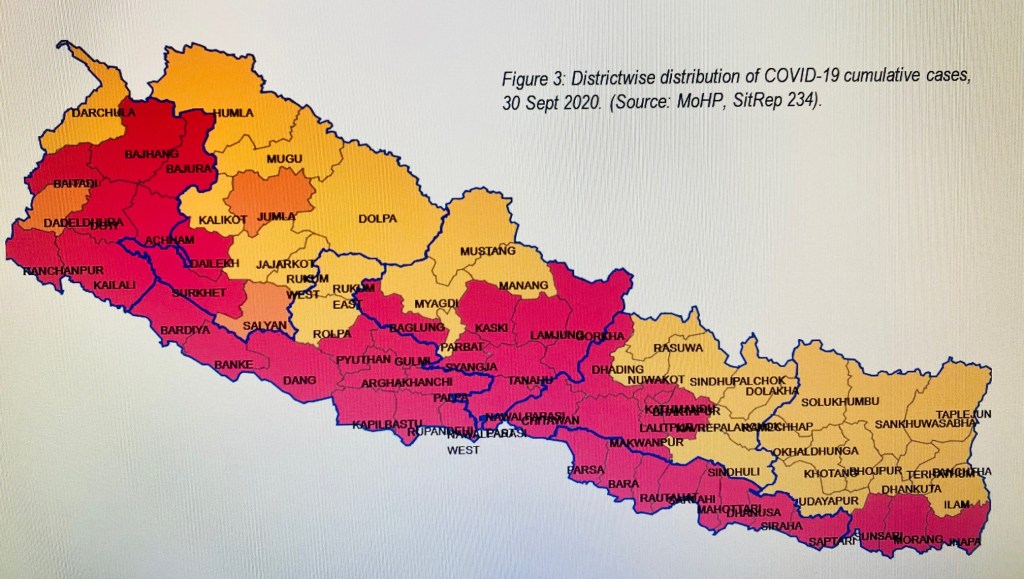
In the following three months, by 30 September 2020, cumulative positivity rate increased less than 2 per cent, to 7.6 per cent. However, the 1 million RT-PCR test showed 77,817 positive cases which was 82.6 per cent increase from June end. Similarly, the death toll also rose steeply, by 82 per cent from June end (Figure 3).
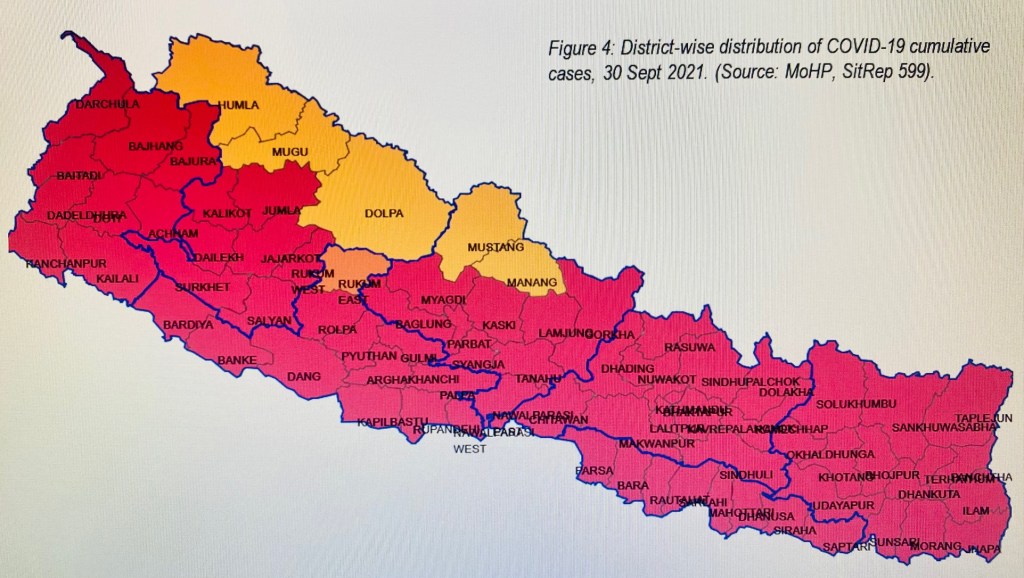
Nepal continued suffering more with the rise of the second wave of pandemic. 717,244 new cases of COVID-19 were reported between October 2020 to September 2021 increasing the death by 90 per cent, 10,637 more than last September. Cumulative positivity rate rose to 18.9 per cent while 3.1 million people underwent RT-PCR test (Figure 4).
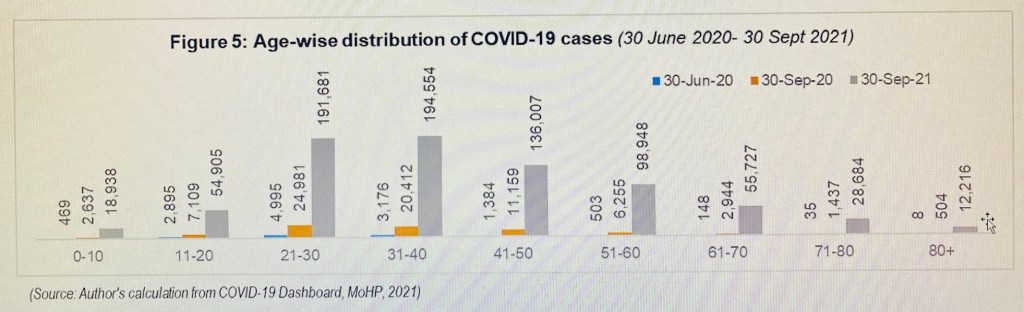
In terms of age-wise distribution of COVID-19 cases in Nepal, people from 21 to 30 age group suffered the most until 30 June 2020. Of 13,613 positive cases, almost 37 per cent belonged to this age group. People belonging to 31-40 age group referred to 23.3 per cent and 11-20 age group occupied 21.3 per cent of the total cases during the same period. The pattern kept changing as the number of cases rose in the following months. Decline among the 11-20 age group was the most remarkable as the distribution of COVID-19 cases between 30 June 2020 and 30 September 2021 reduced by 14.3 per cent.
The change is largely due to the nationwide lockdown which kept the school and college going children and adolescents at home. On the other hand, there were 8.8 per cent increase of cases among the people, referring to 51-60 age group during June (2020) to September (2021). However, the increase was reported 15.8 per cent during the same period to the people belonging to 41-60 age group followed by 9.3 per cent increase of cases among the people from 61 to 80 years’ age (Figure 5). From a gender perspective, while positive cases declined from 89 per cent by June end 2020 among the men to 59 per cent by September end 2021, the pattern reversed for women- 30 per cent rise by the end of September 2021.
While 26 death was reported by the end of June (2020), the number of human casualties increased to 11,135 by September 2021. However, recovery rate rose from 93.7 per cent to 96.3 per cent during this period. The first death from COVID-19 in Nepal was a 29-year-old pregnant woman, on 14 May 2020. By 24 June 2020, the overall case fatality ratio (CFR) across all ages was 0.24 per cent, population over 60 age suffered from highest CRF, 3-8 per cent[3]. CFR which was below one per cent for age group under 54 years by September in 2020 showed a change in pattern by the following September (2011). For example, the fatality rate of 0.09 for the age group 15-24 years in September 2020[4] increased to 0.14 per cent by September 2021[5]. An increase was observed among the age group of 25-54 years during this time interval.
While CFR remained around 5 per cent for 65-74 years’ age group, there was over 2 per cent increase in the age group referring to 75-84 years old, from 7.21 per cent in September 2020 to 9.26 per cent by the following September. Analysing the pre-existing conditions as contributing factor to complicating COVID-19 case, 67.1 per cent, or 329 out of 490 deaths by the end of September (2020) had at least one or more known comorbid conditions. The number halved as only 30.8 per cent (3,415 persons) of death by September end (2021) had at least one known comorbidity.
Since the COVID-19 outbreak, people living with non-communicable diseases (NCDs) opted to be more vulnerable to becoming severely ill or dying from COVID-19. The vulnerability before COVID-19 increased by the presence of underlying comorbid conditions, in particular the NCD conditions such as hypertension, diabetes, cardiovascular diseases, respiratory diseases, cancer, kidney dysfunction, liver diseases, and other immunosuppressive conditions. While it is a bit of difficult for not having enough information for concluding the magnitude of affect due to pre-existing medical conditions and their contribution in COVID-19 associated vulnerabilities, there are studies that indicate a direct link between pre-medical conditions with COVID-19 casualties. One assessment showed that lockdown did also impaired people with NCDs accessing the health facilities and care[6] and further increasing their risk. There were several reports across the country citing the obstruction in assessing the health facilities due to the restriction in movement, response measures, and social stigma about the affected people[7] [8].
With the spread of COVID-19, Nepal kicked-off several initiatives- clinical and non-clinical- to respond against the pandemic. In terms of clinical measures, Government of Nepal adopted numerous policy and intervention measures. Soon after getting the first case of COVID-19 reported on 23 January 2020, a surveillance desk was first opened in the international airport in Kathmandu with an aim of screening the incoming passengers from aboard. Similar type of desks were also also opened in other domestic airports as well as Points of Entry (PoE) with India and China. Quarantine and isolations centres were established in public buildings such as schools and community places. Health facilities, including testing labs, were designated with different levels based on the capacity, and availability of services[9]. Local levels groups were established to ensure contact tracing, including the Case Investigation and Contact Tracing Team (CICTT). Government of Nepal (GoN) launched the vaccination campaign on 27 January 2021. An initial estimate of US$452.8 million was required to fund the national vaccination programme[10] targeting 71 per cent of the population, i.e. 21 million people. The government set a list of priority groups for the vaccination. 7,456,384 received a single dose, and 6,285,740 received a second dose covering a 28.9% of the targeted population by the end of September 2021[11]. Nepal’s vaccination programme, however, is critically relied on India and China to fulfil its vaccine needs[12] later supplemented by COVAX[13].
Non-clinical measures to tackle the challenges COVID-19 has posed, Nepal follows a trial and error method. Nepal has recently adopted to federalism and powers and resources are shared between three levels of governments. However, fragility of the newly restructured public institutions, resource constraints, poor health infrastructure, and lack of a political culture to collectively conceive, prepare and deliver policies and plans have seriously impaired the good intentions in terms of tackling COVID-19 and associated challenges. Various policies are formulated in reponse to COVID-19 since the emergence of pandemic in the country. To coordinate the efforts, a High-level Coordination Committee for the Prevention and Control of COVID-19 was formed on 1 March 2020. The committee was later turned into a Corona Crisis Management Centre (CCMC), a similar mechanism was rolled out at the provincial, and district levels across the country. The emergence of CCMC, however, was criticised by many as an attempt of federal government to erect a parallel structure at the subnational levels undermining the role of the latter granted by the constitution[14]. In July 2021, the federal government tabled an ordinance, COVID-19 Crisis Management Ordinance 2021, in the parliament as a legal remedy to integrate and manage the COVID-19 response measures in the country. However, the ordinance could not get legislative endorsement because of the dissolution of the same. As a result, federal, provincial and district level CCMCs became invalid[15] posing further complexity in the uniform response against COVID-19. Studies also found that relevant agencies, such as the Ministry of Health and Population (MoHP) could play better roles in dealing with the pandemic response[16].
Managing resources to fight against the pandemic is another major challenge for the country. In May 2020, the UN Country Team (UNCT) in Nepal unveiled first preparedness and response plan to respond to COVID-19. The plan sought for US$108.4 million for preparedness and response[17]. Eight months later, on January 2021, another funding appeal for US$49.4 million was made[18]. Within four months later, US$83.7 million was projected in a series of funding appeal since the beginning of pandemic in Nepal[19]. Government of Nepal (GoN) launched a National Relief Programme (NRP) in May 2020 to minimise the effect of COVID-19 and advance socio-economic development. US$1.26 billion was estimated for NRP with US$347 million for health, US$359 million for social protection of the poor and vulnerable, and US$555 million for economic relief package[20]. There is, however, a lack of a robust and transparent system to track how much fund was asked, raised, and spent in the preparation and response to COVID-19 in Nepal. The Ministry of Finance (MoF) reported US$ 599 million foreign aid disbursement by the end of September 2021[21].
Another non-clinical measure against the COVID-19 was restriction of movement, commonly known as ‘lockdown’. A nationwide lockdown was imposed on 24 March 2020 and lifted on 22 July. Some restrictions, however, remained intact until 16 August 2020. During lockdown, domestic and international travels were restricted, points of entry were closed, schools and businesses were prohibited, leaving some essential health and supply services minimally operational. As the second wave of pandemic hit the country, government imposed another series of lockdown in Kathmandu on 28 April 2021, and allowed the district authorities to assess the situation and decide on the restriction measures. The new variants of virus proved more contagious during the second wave of COVID-19 in Nepal pushing the country to the extremely difficult situation as the hospitals ran out of beds, oxygen, and other basic amenities. Infection was widespread in the communities, infected were forced to remain self-isolated, and those in dire need of health service had to queue for their term as chaos became the normal[22]. The lockdown was extended on 16 June 2021 as the second wave of coronavirus surged. The lockdown was lifted on 1 September 2021, though certain restrictions remained enforced. While lockdown measures helped governments’ effort in dealing with the pandemic, in particular the spread of infection beyond control, the people had to pay a hefty price. Studies found that lockdown had a multidimensional impact on society, including the effect of health of individuals and disruption in healthcare services[23].
Coronavirus has made a significant impact on all lifestyles and in all communities across the world. With the emergence of new mutants and their affects on society are yet to be adequately measured. A country like Nepal with fragile public sector institutions, weak health infrastructure, and complex socio-economic realities, COVID-19 has led to further implications for the country and its 29 million population. With collaborative efforts, increased transparency, accountability, and inclusion of all with stakes can, however, make the response more robust and recovery goals more realistic. COVID-19 has also provided a great opening before the country to learn lessons and adopt appropriate policy measures to prepare for future emergencies with an aim of minimising the human and economic losses and recover quickly.
[1] Ministry of Health & Population (MoHP), 2021. SitRep # 599, Kathmandu.
[2] Government of Nepal (GON), 2020. SitRep #01, Kathmandu.
[3] WHO, Nepal SitRep #9, 24 June 2020.
[4] WHO, Nepal SitRep #24, 30 September 2020.
[5] WHO, Nepal SitRep #76, 30 September 2021.
[6] WHO, 2020. Rapid assessment survey of service delivery for NCDs during the COVID-19 pandemic. May 2020.
[7] Gupta, TK, 2020. Social stigma during COVID-19 pandemic, published in The Himalayan Times, 9 April 2020 and available at https://thehimalayantimes.com/opinion/social-stigma-during-covid-19-pandemic.
[8] ICJ, 2020. The Right to Health: Redirecting the “Unconstitutional Path” of Nepal’s COVID-19 Responses. A Briefing Paper, November 2020.
[9] MoHP, 2020. COVID and Other Health Service Delivery in the Context of COVID-19 Pandemic- Interim Directives, 2020. Available at https://drive.google.com/file/d/1kzWQTtyi2cz8HSA4Hwv3zjdHwExJQXhO/view
[10] ADB, 2021. Vaccine Needs Assessment. Responsive COVID-19 Vaccines for Recovery Project under the Asia Pacific Vaccine Access Facility. Available at https://www.adb.org/sites/default/files/linked-documents/55084-001-sd-01.pdf
[11] MoHP, 2021. SitRep #599, 30 September 2021. Available at https://covid19.mohp.gov.np/covid/englishSituationReport/6155a3246c93a_SitRep599_COVID-19_30-09-2021_EN.pdf
[12] Kuronuma, Y, 2021. Nepal’s Oli wants China and India to step up with vaccines ‘first.’ Published in Nikkei Asia, 21 May 2021. https://asia.nikkei.com/Spotlight/The-Future-of-Asia/The-Future-of-Asia-2021/Nepal-s-Oli-wants-China-and-India-to-step-up-with-vaccines-first
[13] Poudel, A, 2021. With COVAX under pressure, Nepal’s vaccine crisis deepens. Published in The Kathmandu Post, 18 May 2021. https://kathmandupost.com/health/2021/05/18/with-covax-under-pressure-nepal-s-vaccine-crisis-deepens
[14] Pradhan, T.R., 2020. Given its failure, Covid-19 Crisis Management Centre’s relevance is questioned. Published in the Kathmandu Post on 7 October 2020. Available at https://tkpo.st/3jFoZGt
[15] Pradhan, T. R. & Prasain, S. 2021. Big Confusion as top body responding to COVID-19 becomes defunct. Published in the Kathmandu Post on 18 September 2021. Available at https://tkpo.st/2VStqXW
[16] NHRC_2021. RA of COVID-19 Related Policy Audit in Nepal_ Nov 2020.
[17] UNCT, 2020. COVID-19 Nepal: Preparedness and Response Plan (May 2020). Available at https://reliefweb.int/report/nepal/covid-19-nepal-preparedness-and-response-plan-may-2020
[18] UNCT, 2021. COVID-19 Nepal: Preparedness and Response Plan, Revision (January 2021). Available at https://reliefweb.int/report/nepal/covid-19-nepal-preparedness-and-response-plan-cprp-january-2021
[19] UNCT_ 2021. Nepal: COVID-19 Response Plan, issued 20 May 2021 (for the period May 2021 – August 2021). Available at https://reliefweb.int/report/nepal/nepal-covid-19-response-plan-issued-20-may-2021-period-may-2021-august-2021
[20] MoF, 2021. COVID-19 Active Response and Expenditure Support (CARES) Program. Third Semi-annual Report, August 2021.
[21] Ministry of Finance (MoF), 2021. COVID-19 Assistance Portal. Calculation is made by the author based on the available figures in the portal on 25 October 2021. Detail can be assessed at https://amis.mof.gov.np/web/guest/covid-19
[22] Pandey, L. 2021. COVID: Nepal reeling from a deadly second coronavirus wave. Published in DW on 7 May 2021. Available at https://p.dw.com/p/3t6GN
[23] Sharma, K.; Banstola, A.; and Parajuli, RR. 2021. Assessment of COVID-19 Pandemic in Nepal: A Lockdown Scenario Analysis. Front. Public Health 9:599280. doi: 10.3389/fpubh.2021.599280.
